
In this blog post, we examine paid claims data from a large, nationwide employer plan to understand the impact that COVID-19 has had on healthcare claims. We also consider some of the sources of uncertainty that health plans are dealing with in forecasting claims in the face of this evolving pandemic.
In early March, as the United States began coming to grips with the potential impact of the COVID-19 pandemic, many healthcare providers put a pause on elective procedures and shifted their focus from normal operations to preparing to care for COVID-19 patients. At the same time, Americans began avoiding emergency rooms, physicians’ offices, and other health care settings, fearing the risk of infection. To date, in most of the country, the cost savings from this foregone care have generally exceeded the cost of treating COVID-19 patients. As a result, many health plans have seen their margins increase. Some health plans are responding by offering premium discounts, waiving cost sharing for the treatment of COVID-19, and working to support providers, or a combination of the three. Health plans may be taking these actions, at least in part, to avoid having to pay medical loss ratio rebates under the Affordable Care Act.
At the same time, there is considerable uncertainty regarding the cost and utilization of healthcare services going forward. There is uncertainty regarding the potential for additional waves of COVID-19-related illness, the cost associated with treating the residual effects of those recovering from COVID-19, the timing, efficacy and cost of any vaccine, the cost of continued testing, the impact of non-COVID-19 patients who delayed care and therefore present with more advanced disease, and there is uncertainty around how much of the care that has been foregone, say joint replacement surgeries, will ultimately return.
In its 2Q 2020 earnings call, UnitedHealth Group’s CFO, John Rex, noted that “At the lowest point in April, in-patient care, inclusive of COVID-19-related care, was about three-quarters of baseline. In June, this recovered to nearly 95%.” He further noted that “These national trends have continued thus far in July even as certain states are seeing short-term deferral of services where there are elevated levels of infection and hospitalization.”
We have been given access to a dataset of healthcare claims from a large, nationwide employer. This employer has employees in every geographic region and a stable workforce with limited exposure to layoffs and furloughs that have occurred to date. In the chart below, we show this employer’s weekly paid claims for both the first 28 weeks of 2019 and the first 28 weeks of 2020, all relative to the average weekly paid claims in 2019.[4]
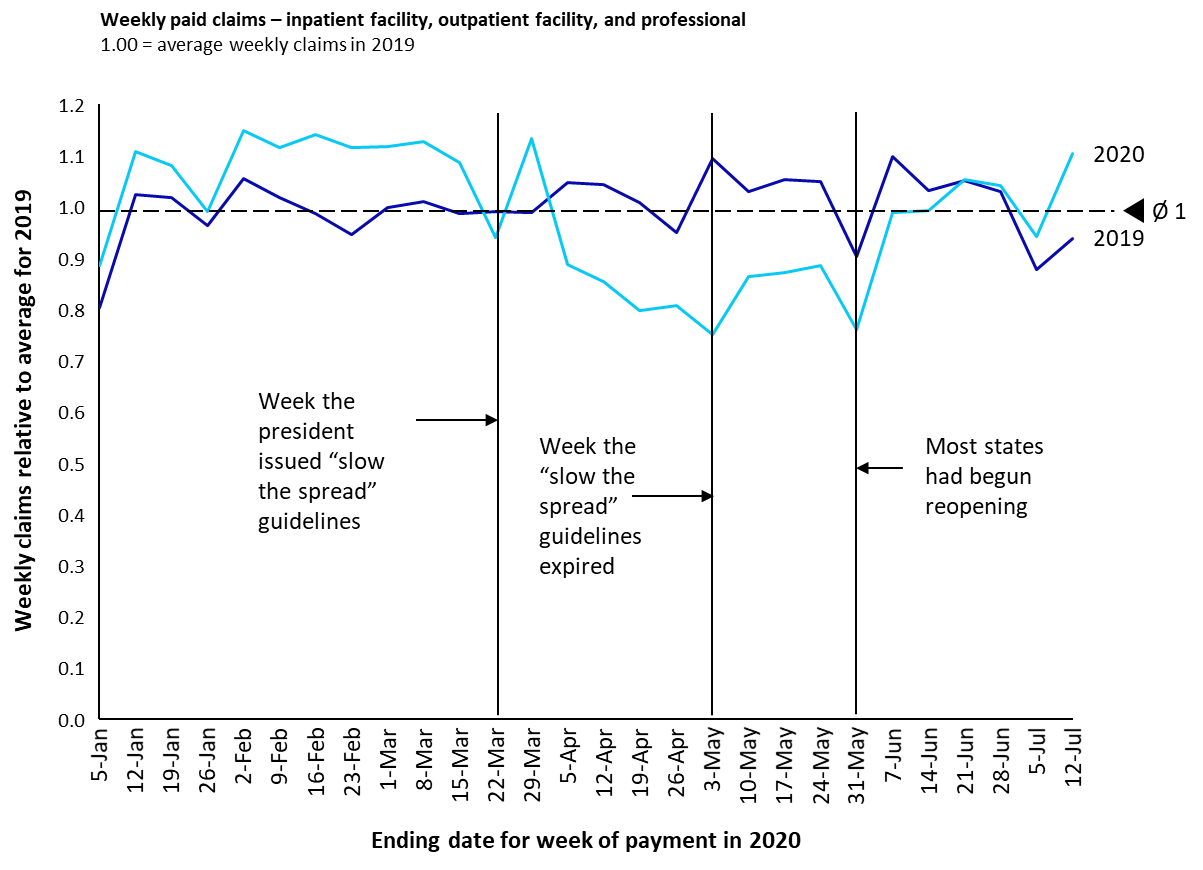
The first week in our data for 2019 runs from December 31, 2018 through January 6, 2019. The first week in our data for 2020 runs from December 30, 2019 through January 5, 2020. The remaining 27 weeks follow accordingly.
Note that there is a lag between the time services are provided and claims are paid. That lag will vary by type of service, and by issuer (some issuers pay a larger share of claims based on electronic edits, and therefore more quickly, than others).
Between the week ending January 5, 2020 (week 1 of 2020 in our data) and the week ending March 22 (week 12), weekly paid claims in 2020 averaged 109% of weekly paid claims in 2019. On Monday, March 16, the president issued a set of guidelines that Americans were to follow for 15 days to “slow the spread.” The president later extended those guidelines for another 30 days to expire on April 30. As the chart shows, and keeping in mind the lag between a service being provided and the claim being paid, the impact on paid claims was rapid and negative. Between the week ending March 29, and the week ending May 31, average weekly paid claims in 2020 were 15% below average weekly claims for the same period in 2019, reflecting the impact of deferred and foregone care following the shutdown. With the president’s guidelines expiring on April 30, three states, Georgia, Oklahoma, and Alaska, began reopening, allowing some personal care businesses, dine-in restaurants and theaters to reopen. The reopening was gradual, but by the middle to end of May, most states had begun to reopen. From the week ending June 14 through the week ending July 12 (week 28), the most recent week of detailed data we have available, paid claims in 2020 were 4% above claims for 2019. Our hypothesis is that this reflects the beginning of the return of care that had been delayed. If the pattern in the last two weeks of data were to persist for the balance of the year, and early indications are that that pattern will, paid claims for all of 2020 would be roughly 6% higher than paid claims for 2019.
It is possible that paid claims will be suppressed in the second half of 2020 as many parts of the country are experiencing increasing cases of COVID-19. At the same time, the cost of treating new COVID-19 patients coupled with the return of care that had been delayed could push paid claims higher than those we see in the data when the states began reopening. Health plans, providers, regulators and policymakers will be keeping a close eye on how this develops.
###