Cell and gene therapies provide a unique opportunity to transform patient outcomes, especially for those with the highest need and where current treatment options do not suffice. Cell therapies such as the CAR-Ts have launched as a last-line option in haematologic conditions whereas gene augmentation therapies are now being used as the main treatment option for some rare diseases. With an estimated 80% of rare diseases having a genetic component, these conditions will be the drivers of gene therapy use and uptake. In both instances, often the patient eligible for such a therapy needs to be treated as early as possible to benefit most.
The need for earlier patient identification
Studies suggest that it can take between four and five years on average to be diagnosed with a rare disease, with some over 10 years. Time is of the essence to ensure these therapies can be provided as early as possible, especially in patients where a delay can make a patient’s use of therapies inappropriate or potentially outside of eligibility requirements. A case example is a condition such as Duchenne muscular dystrophy where it can take one to three years from symptom onset to diagnosis. For patients with a fast-progressing condition, that timeline can result in a significant proportion of children becoming non-ambulatory. Today, roughly 40% of rare disease patients point to misdiagnosis as a key reason for delayed treatment, with treatment delays also being driven by the lack of defined referral pathways and the time it takes to get coverage approval in markets like the United States. From a cell therapy perspective, some estimates suggest that approximately half of the patients eligible for cell CAR-T may get therapy. Early referral and coordination between chemotherapy physicians and CAR-T centers are critical to ensure that patients eligible for cell therapy do not face delays and are not treated with therapies with strong toxicity that may lead to their cells being damaged for future autologous transplant or CAR-T.
Moving from diagnosing to predicting
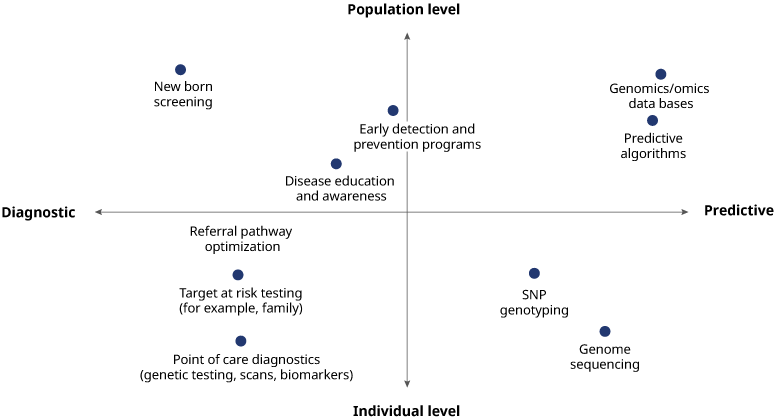
Appropriate patient identification is a multi-faceted approach and solutions will vary across geographies and conditions. Historically, patient identification strategies have been diagnostic, whether it is point-of-care testing for an individual or at-risk testing for groups. The process has largely been driven by pharmaceutical companies. At a population level, this often translates into individual companies working with healthcare systems to implement different testing programs for the same disease. Such a fragmented approach is inefficient and unsustainable financially. Prolonging this approach will hurt the industry and patient care, making future research more difficult with siloed datasets sitting across competing private interests.
In our roundtable with industry leaders across biopharma, payer, and provider Organizations, we explored taking a more predictive approach that builds an earlier understanding of patient populations, including a clear view of epidemiology within and across geographies. Doing this at scale requires building large population databases and relying on machine learning and artificial intelligence to hasten knowledge of individual risk and to target interventions.
How and when to apply robust predictive analytics depends on the condition and demands a clear understanding of disease pathology and phenotype-genotype correlations. As an example, within LSD conditions, Gaucher represents a better starting point versus Fabry where there is a greater diversity of mutations leading to greater complexities of phenotype-genotype correlations. For other conditions, newborn screening remains the intervention of choice for such conditions as sickle cell disease and more attention should be paid to making this a priority globally.
Essential to adopting a predictive approach is the utilization of an open-source and open-access database. AI-driven predictive algorithms are being used elsewhere in healthcare to drive population health management and for patient identification. To enable this in cell and gene therapy, the industry and healthcare system must shift from genetic testing for certain conditions to broader testing, as well as leverage whole genome sequencing. The databases need to easily integrate into electronic health record systems and imaging and testing platforms.
To drive this, the roundtable attendees identified a few key success factors:
Building trust and breaking down silos: Healthcare is a highly competitive industry resulting in limited data sharing across all segments. Building a predictive engine requires true collaboration from a multitude of stakeholders, ranging from patient advocacy groups, pharmaceutical companies, researchers, government, and providers. Patient groups are often the most trusted partner in this ecosystem and building around the right partners with the mindset to invest in the journey will be critical.
Solving for consent and privacy management: The proliferation of health data sources and platforms has increased the industry’s ability to collect information, including on patient outcomes. But since individuals own their health data, positively engaging them is critical. Any scalable solution needs to put people at the center of its design architecture. A key aspect of this is ensuring secure digital identifications that are operable across healthcare records and suppliers, requiring a combination of robust pseudonymization and virtual identity verification amongst others.
Rethinking the research versus commercial divide: Although disease registries, biobanks, and federated databases exist, this data warehousing has often been done in research settings, which have strict data and privacy requirements. In such instances, the data is underutilized and there is a need to rethink the divide between research and commercial needs, focusing on a dynamic and flexible approach that puts patients at the center of consent management. For instance, the industry could consider opt-out policies, incentivizing individuals to share data with healthcare tokens, or other forms to drive engagement.
Finance together, not individually: Creating a systemwide solution for data collection and sharing cannot be done in silos or financed by individual stakeholders. Doing so is not only inefficient and costly, but will drive further fragmentation. Incentives need to be aligned across all segments to create a more collaborative financing methodology. Given the number of therapies expected to launch by the end of the decade, continuing with the status-quo approach to finding patients in the system is likely to lead to certain patients missing out on life-changing interventions. Taking the next step requires a collaborative approach and rethinking how we build the systems to identify patients and get them to treatment. Now more than ever, we have the health data and analytics capabilities that can enable this with the right impetus and willingness across stakeholders.
This white paper is an output of a recent cell and gene therapy (CGT) roundtable convened by Oliver Wyman to bring together industry leaders across biopharma, payer, and provider organizations to discuss the need for driving patient identification at scale and realize the benefits of cell and gene therapy.
