After a year of doubt, it seems that Medicare Advantage (MA) is here to stay. Indeed, the Congressional Budget office now estimates that MA will account for almost one-third of Medicare participants by 2023.
But MA plans can’t become complacent: The market is evolving, and CMS has made it clear that it wants better performance and better value out of this very important program. Yesterday’s successes won’t guarantee tomorrow’s survival. To succeed, MA plans need to keep advancing — building consumer value, deeply engaging providers, and ensuring they are “purpose built” to serve seniors.
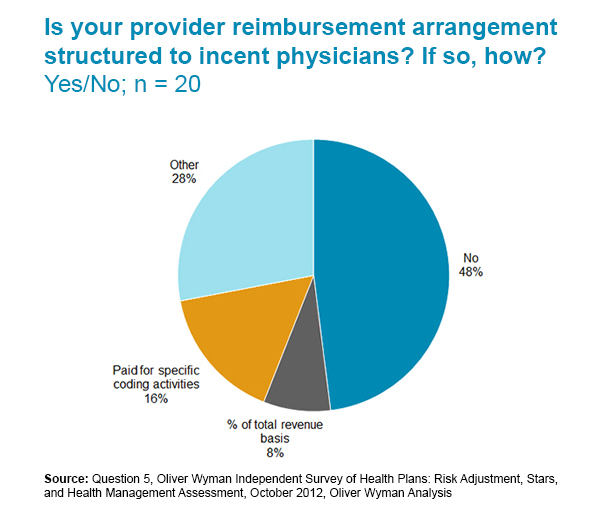
Physician incentives? Half of Medicare Advantage plans don’t use them yet.
Medicare Advantage (MA) plans have a well-earned reputation for being ahead of the pack in adopting value-based care. But there’s still a long way to go. It’s a rare MA plan that has more than one-third of its providers on value-based contracts — more are closer to 10 percent. And physician incentives are by no means universal.